
Commentary|Articles|January 27, 2026
Q&A with Karen McGuire, PhD: How TolaSure Aims to Redefine the Standard of Care for EBS
Listen
0:00 / 0:00
Karen McGuire, PhD, discusses TolaSure, a groundbreaking therapy targeting epidermolysis bullosa simplex, focusing on cellular repair and blister reduction.
Advertisement
As investigational therapies increasingly aim beyond symptom control in rare dermatologic diseases, novel approaches that target underlying cellular pathology are drawing attention.
Dermatology Times: What is TolaSure’s mechanism of action? How does it differ from current EBS treatments, like standard-of-care wound management?
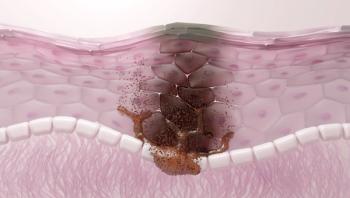
McGuire: So current standard of care is pain, itch, and wound management. We're just trying to control pain and infection. And most of the drugs in development right now are going after those kinds of symptom management modalities, if you will. Our platform is called mTORX and we use those mTOR inhibitors to induce autophagy in the cell. And by leveraging autophagy, we're able to remove a lot of the mutated, misfolded, and damaged keratins out of circulation. And in doing that, we're able to take what were very weak intermediate filament networks inside the basal keratinocytes and strengthen those networks. And that is what's resulting in the reduction in blistering that we're seeing in patients.
Dermatology Times: What were some of the key takeaways from TAMES-01 that support this next step of research?
McGuire: We looked at a variety of end points; global assessments, pain, itch, blistering, erythema, and so forth. And we actually did multi-factor analysis on our data to figure out which of these symptoms is really driving the disease. And we figured out that it was really the blistering that was the key driver. So we measured the surface area of blisters, both intact and ruptured blisters, and we monitored that change over time, and within about 2 to 3 weeks, we were seeing 96% reductions in blister surface area for these patients. In the placebo group, they would get a little better, and then they get a little worse...it's a very dynamic disease. But what we're really excited about is to be able to really interrupt that process, interrupt almost like a flare, if you will, for an EBS patient.
The other key takeaway is that we took some biopsies at the end of the study from both our treated and untreated patients. Under electron microscopy, we were actually able to see these filament networks that I mentioned earlier restored, improvements in those intermediate filament networks, which is key in trying to tie back our mechanism of action to real improvements in patients.
Dermatology Times: How does
McGuire: Again, we're using blister surface area as our main outcome measure. TAMES‑01 was internal controls so TAMES‑02 is 2 distinct groups of patients, either directly on active or placebo. But we designed it in such a way that any patient in the placebo arm can cross over and be put on active after 2 months. So everybody gets to try the medication, essentially. We're really hoping to be able to repeat and be able to see that blister reduction again in these patients. We're going to do an interim readout after about 20 subjects out of the 40 total we have planned for the phase 2. We're hoping to get breakthrough designation for that as well, and then if we can get agreement from the FDA, we'd like to parlay that right into a pivotal phase 3 trial. We're really trying to get this on the market as quickly as we can for patients. We already have orphan drug status and rare pediatric disease status for this indication, and we're really excited.
The TAMES‑02 study is actively recruiting right both at Stanford and at Northwestern. Joyce Teng, MD, PhD, and Amy Paller, MD, are really spearheading this effort for us at those 2 institutions. We do cover all the travel costs and everything to bring patients into these big centers of excellence. If there are physicians out there, and you have quite a few of these patients, and you might be interested in participating in our phase 3 pivotal trial, please let us know. We're interested in talking to any dermatologists and groups that may have patients who would benefit from this therapy. We're also looking for the right partner to really help us get it to commercial as quickly as we can. We want to try to get this drug to as many patients as possible.
[Transcript has been edited for clarity]
Advertisement
Related Content
Advertisement


Latest CME




Advertisement
Advertisement
Trending on Dermatology Times
1
BBT001 Bispecific Antibody Demonstrates Fast AD Clearance and Long-Lasting Itch Relief in Phase 1 Trial
2
The Aesthetic Edge: July 2026
3
Dermatology Times July 2026 Recap
4
UV Safety Awareness Month 2026: The Latest Research, Trends, and Clinical Insights
5