Now Playing
James Q Del Rosso, DO, Raj Chovatiya, MD, PhD, Lisa Swanson, MD, provide an overview of atopic dermatitis and review the burden of disease.
James Q. Del Rosso, DO: Hello, I’m Dr Jim Del Rosso, and welcome to this Dermatology Times® Between the Lines. Today we’re going to feature a discussion of an article, “Rapid Pruritus Reduction With Ruxolitinib Cream Treatment in Patients With Atopic Dermatitis.” I’m a dermatologist based in Las Vegas, Nevada. I’ve been here for 26 of my 36 years of practice. I also run a clinical research center, and I’m involved in a lot of educational initiatives. Atopic dermatitis has always been an academic interest and a research interest of mine. I’ve been an investigator with ruxolitinib [Opzelura] cream. Hopefully we’ll bring to light some important information.
Raj Chovatiya, MD, PhD: My name is Dr Raj Chovatiya. I’m an assistant professor of dermatology, the director of the Center for Eczema and Itch, and the medical director of the clinical trials unit at the Northwestern University Feinberg School of Medicine in Chicago, Illinois.
Joining me is 1 of my best friends in the world, my colleague Lisa Swanson, an all-around super genius and a pediatric dermatologist at Ada West Dermatology in Boise, Idaho. Lisa, thanks for joining me.
Lisa Swanson, MD: Thanks for having me, Raj.
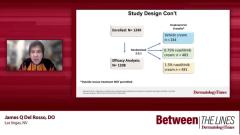
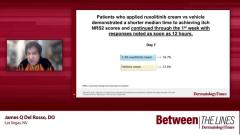
James Q. Del Rosso, DO: We’re going to focus on the practical and clinical implications of itch based on phase 3 pivotal trials, TRuE AD1 and TRuE AD2, because itch is a significant problem in patients with atopic dermatitis. Atopic dermatitis usually starts early in childhood and rears its head throughout the adolescent years and frequently into the adult years. There may be periods where it quiets down, and we don’t see patients as much with significant flares. But on a chronic basis, almost every day, patients have dry skin and low-grade eczematous dermatitis, so itching is a significant problem.
It affects them and everybody else around them. If it’s someone’s child, it is hard to watch and keeps everybody up at night. It’s a very difficult problem. We’ve had a lot of therapies for atopic dermatitis, both topical and systemic, but sometimes the effect on itch is not as much as the patient would like, especially early on. Some therapies can do that.
Raj Chovatiya, MD, PhD: I’m glad we get to talk about atopic dermatitis together because that’s 1 of my favorite things that we get to do. I want you to unpack for us about the burden of quality-of-life issues when it comes to this disease.
Lisa Swanson, MD: It’s huge. You only have to spend a couple of moments with your patients with atopic dermatitis to know how badly they’re suffering. The itch is nonstop. It disturbs their sleep, their happiness, and the activities they enjoy. It’s a huge deal.
Raj Chovatiya, MD, PhD: You talked about that itch part. That’s probably the most distressing, stressful, bothersome symptom, and study after study reflects that. That itch is connected to sleep and mental health issues, particularly in children. There are even reports of conduct disorder, learning-related issues, and ADHD [attention-deficit/hyperactivity disorder]. Some studies even suggest suicide attempts.
Lisa Swanson, MD: Absolutely. Individuals scratch so much, it’s to the point that they’re bleeding. They prefer the pain of that to the itch they feel. Itch is a profound symptom.
Raj Chovatiya, MD, PhD: Do the rates of itch differ significantly across demographics in your patients—men, women, racial groups, where individuals live, etc? Do you feel the burden is pretty similar? Any insights you have there?
Lisa Swanson, MD: It’s pretty similar. Climate can play a role. I’ve practiced in Colorado and Idaho, which are both pretty dry states. We see a lot more itchiness and a lot more atopic dermatitis because of our climate. That may play a role. But demographically, anybody with atopic dermatitis deals with itch.
Raj Chovatiya, MD, PhD: In the studies I’ve seen, a lot try to break these things down into racial and ethnic groups, which admittedly are sociopolitical constructs and not biological constructs. But it seems many groups oftentimes have poorer access, poor insurance, and don’t get to a dermatologist. Their disease is much more severe. Therefore, their burden of itch ends up being that much higher. It behooves us to think about those things whenever anyone comes in, especially the ones who have been disconnected from care, and the itch is affecting their lives.
Lisa Swanson, MD: Definitely. Especially if they don’t have access to good care, then they’re more likely to show the long-term manifestations of being itchy and scratching: lichenification, dispigmentation. You’re going to see more of those things in that patient population.
TRANSCRIPT EDITED FOR CLARITY