Now Playing
Joshua Zeichner, MD, and Mona Gohara, MD, discuss how adherence becomes an issue in the treatment of acne and what factors lead to lack of adherence in patients.
Joshua Zeichner, MD: Hi everybody, welcome to this Dermatology Times® Between the Lines presentation titled, “The Role of Nonprescription Products in the Management of Acne.” I’m Joshua Zeichner. I’m an associate professor of dermatology at Mount Sinai Hospital in New York City, and I’m joined by my good friend Mona Gohara, who is a dermatologist at Dermatology Physicians of Connecticut in Hamden, Connecticut, and the president of the Women’s Dermatologic Society. Mona, thank you for being here.
Mona Gohara, MD: Josh, thank you for having me and thanks to Dermatology Times® for having me. This will be an exciting and fun discussion.
Joshua Zeichner, MD: Our discussion today is going to talk about challenges patients experience in adhering to their acne treatments. We’re also going to review updates on the available moisturizers and cleansers for patients with acne and discuss factors that shape the selection of appropriate adjunctive therapy in treating our patients who are prone to acne. Let’s get started.
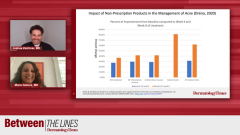
Let’s start with findings from a 2019 study suggesting that nearly half of patients stop their topical acne therapies before they’re supposed to because they are unresponsive to their treatments, or they experience adverse effects. Let’s talk about adherence as being important in treating acne and why it’s a challenge. What are the difficulties you’re experiencing with your patients?
Mona Gohara, MD: I wasn’t shocked by this number. You are an acne expert and as we know clinically, patients will often come in and say, “It didn’t work, or I stopped using it, or I’m allergic to it.” We know it’s just more of an irritant dermatitis. We’ve discussed this before, retinoids and benzoyl peroxide for comedonal acne, and for some component of inflammatory acne, these are the gold standard. We don’t want to stop using them because they’re efficacious and we know that they can help our patients. As it pertains to the issue of adverse effects, which happens a lot, I wonder because in the study the authors did point out that when the patients were using the medications QD [every day] as opposed to BID [twice a day], or when the patients were using the medications every other day as opposed to every day, the adverse effect profile decreased in terms of irritants. I wonder Josh, are we taking the time to slow down, talk to our patients and say here is how much you have to use with a retinoid, a pea size amount, over your whole face, the whole spiel, moisturize after you use it, work up gradually. I hand my patients a handout that talks about optimal retinoid use or take a picture of it and text it to them because then they can have it on their mirror, and they can use it on a day-to-day basis. A lot of the irritation would subside if we communicated clearly about gradual work up to using it and using only a small amount.
In terms of unresponsiveness, you and I both know that sometimes people have unrealistic expectations, both in terms of how quickly the medication is supposed to respond—if you think your acne medication is supposed to respond as quickly as you can get an Uber Eats burger, that’s not going to happen. Also, in terms of the type of acne and topical medications, if you are dealing with severe inflammatory or cystic acne and the patient does not want oral medications, of course, they are not going to be responsive to it and they may discontinue it. Setting up expectations in terms of when you should see a response is important. I tell my patients over a 3-month course, “Hey, I will see you back in 6 weeks.” At that point, we may see 20% to 30% improvement, and that would be considered a good response. If you come back in 6 to 8 weeks and you had zero improvement, that is not a good response. To me, a lot of this could be mitigated, and I would love to hear your opinion as the expert. A lot of this can be mitigated with communication and setting the stage for expectations.
Joshua Zeichner, MD: I agree with everything you just said, and this is where the art of medicine comes in as opposed to just the science. There’s a big difference between giving a patient a prescription for a topical retinoid or benzoyl peroxide and saying, “Use it, and then I will see you, and it will work.” As you said, you have to set expectations, give specific guidance on how much to use, how often to use it, and what over-the-counter products you should combine it with. We know that topical retinoids and benzoyl peroxide are probably the 2 most effective ingredients that we have to give patients by prescription topically. But they are associated with significant irritation more than others, so combining with appropriate gentle hydrating cleansers that won’t disrupt the skin barrier, combing it with moisturizers can reduce the risk of irritation. Telling patients how much to use, I am sure you say the same thing that I say about a green pea-sized amount or a chickpea, or I’ll say, “A green pea, if you have to use 2 green peas that’s fine, but cherry tomato is too much, you know you are using way more than you need to.” We should be starting out every other day, so patients can acclimate to the medication, especially when we are talking about topical retinoids.
As you said, setting expectations on time to improvement. Consumers and patients want improvement over night, but the reality is that the primary end points in clinical trials for prescription acne medications are usually at that 12-week mark, and there are always data that we have after 3 or 4 weeks, but patients are not going to get that immediate overnight improvement that many are expecting. We also have to make sure patients are using the medications. I always say to patients when they come back, first of all, “how do you feel about your skin?” I like to hear what they have to say before I make a comment. I will say to them, “take me through your regimen;” I always ask open-ended questions. I am sure you have people who say, “my face isn’t [improving], the medicine is terrible.” Did they have the chance to pick it up from the pharmacy? Sometimes, they don’t. We have to be nonjudgmental, educate our patients, and set realistic expectations.
Mona Gohara, MD: Absolutely. I had an attending [physician] in residency who said if they are not responding to the medications, if they are not better, it’s 1 of 3 scenarios: it’s the wrong diagnosis, they are not using the medication, or it’s the wrong medication. These questions you have to ask, sometimes they are not using the medication.
Joshua Zeichner, MD: Do you have any other tips that you have specifically on retinoids or benzoyl peroxide? The biggest risk, biggest reward; go ahead.
Mona Gohara, MD: For retinoids, you bring up an important point, which I know I will be talking about a bit later, is what are you mixing it with, how is this fitting into your routine? Are you slathering on an alpha hydroxy acid before or after? Are you doing some type of extreme exfoliation before or after? I like to often times mix it.
Joshua Zeichner, MD: What about the drying toners because those are my favorites?
Mona Gohara, MD: Yes. The third thing we have to ask our patients in addition to how much and how frequently are you using it is what else are you using it with? Lord knows, there is a whole armamentarium of acne medications that people feel like they can just grab off the shelf or the latest YouTube recommendation. And only some of what we’re saying is going into their routine, but it’s being admixed with all this other stuff. Also, it’s important to encourage them oftentimes, if it’s too irritating, to cut it with a cream, to mix it with a cream as they are using it, so that it helps to mitigate irritation. You know what else, Josh, people use retinoids as spot treatment.
Joshua Zeichner, MD: It will dry you out, but it’s not going to treat the acne.
Mona Gohara, MD: Yes. They think it’s not getting better and it becomes extremely irritating, so one of the first things I say to them is this is not a spot treatment. I will use some benzoyl peroxide products as spot treatments….
Joshua Zeichner, MD: Yes, 100%.
Mona Gohara, MD: Again, every medication has a role in the acne armamentarium, and we have to be very clear about, through communication and sometimes demonstration in the office, what we expect from these medications and letting them know that some irritation may be normal. It’s OK. That doesn’t mean that the first time you get a little scaly patch on your face, that’s grounds for discontinuation.
Joshua Zeichner, MD: Yes.
Transcript edited for clarity